

Welcome to SS White's Endo Academy
Learn more and explore with our ever-growing library of clinical cases below, all about Endodontics. Everything is user-friendly! We designed the Endo Academy to provide value and growth for you and your practice.
Clinical Cases
View some recent cases featuring SS Whites products below.
 |
Dr. Solomonov
Michael Solomonov, DMD, is an Israeli board certified endodontist and the director of the Postgraduate Endodontic program in Endodontics at the Sheba Medical Center, Tel-Hashomer, IDF, Israel. Dr. Solomonov received his DMD degree at the Tel Aviv University in Israel in 1994, and in 2002 graduated from the 3 years postgraduate program in Endodontology at the Hebrew University – Hadassah in Jerusalem. From 2008 Dr. Solomonov is an examiner for the Israeli Board of Endodontics at the Scientific Council of the Israeli Dental Association. |
Case#1:
Tooth #27
44 years old male patient presents with Irreversible PulpitisOne S shaped MB canal,Oval cross section WL .Length 26mm.
DB 26mm length
Instrumentation of MB'DB: Glide path\scouting by 06,08,10 SS K-File
+ DCTaper 13,17,20.06,25.06.30.06 Length 31
P canal WL 28 mm Instrumentation: Glide path\scouting by15 SS K-File+ DCTaper 20.06,25.06,30.06,35.06 length 31
SAF was used in MB and P canal as Final preparation.
Combination technique of obturation: Gutta-percha and BJM RCS
Temporary filling : Coltozol,IRM
 |
 |
 |
 |
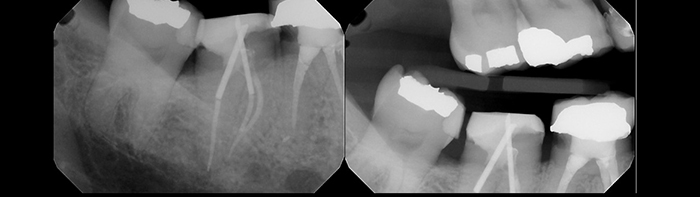
Case#2:
46 years old man Tooth 37. Presents with painful irreversible Pulpitis. One visit treatment. Mesial Canals Glide Path/Scouting by 06,08,10 SS K-Files and 13,17,20.06,25.06,30.06 DCTapers with preservation of S shape form and without sacrificing PCD.D canal Glide Path/Scouting by 15 SS K-File and 20.06,25.06,30.06,35.06 DCTaper Instruments were of 25 mm length and were pre-curved because of patient inability to open the mouth more than 30 mm. Obturation by combination of Lateral and Vertical compaction. Sealer is BJM RCS( Epoxy sealer with macromolecule for prevention of biofilm formation). Temporary filling : Double seal byb CAVIT and IRM. |
 |
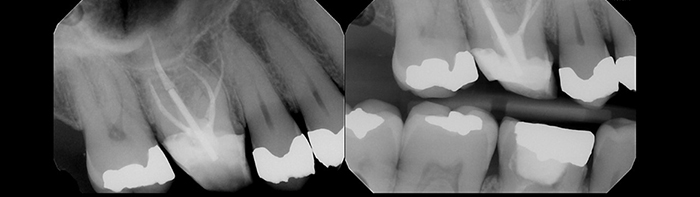
Case#3:
Tooth #16
34 years old female patient referred to RCT after first aid( irreversible pulpitis)One Long Oval MB Canal was prepared by combination of DCTaper 17,20.06,25.06 and SAF system.
DB Canal was prepared by 10 SS K-File and 17,20.06,25.06,30,06 DCTaper.
P canal was prepared by 20.06,25.06,30,06,35.06 DCTaper.
Irrigation by NaOCL 3,5%
COMBINATION TECHNIQUE OF OBTURATION (Lateral and vertical compaction)
Gutta-Percha and BJM RCS
 |
 |
 |
 |
 |
Dr. Reza Farshey
Dr. Reza Farshey received his Bachelor’s degree in Physics in 1994 from McGill University. He then moved to Boston to study dentistry and received his dental degree from Tufts University in 1998. After completing a one-year general practice residency at Berkshire Medical Center, he went on to maintain a successful restorative practice for the next seven years. He was also active in academics as a clinical instructor in the Department of Restorative Dentistry at Tufts University during the same time. In 2005, Dr. Farshey ended his tenure as a general dentist to further pursue his interest in endodontics. He completed his endodontic specialty training at Boston University in 2007 and has been practicing in the Washington metropolitan area since. |
Case#1:
Tooth #29
Diagnosis: Patient presented with a sinus tract in the B aspect of tooth with mild symptoms when chewing. Pulp Necrosis with Chronic Apical Abscess RCT through existing crown, taking care to not over-enlarge dentin that is structurally important to the tooth’s longevity.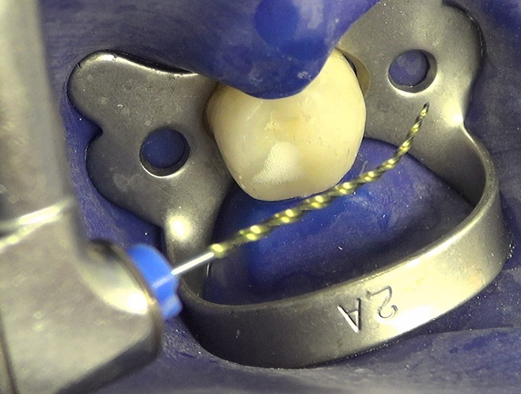 |
 |
 |
 |
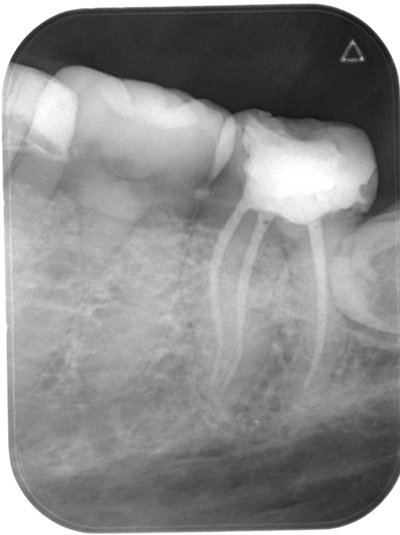
Case#2:
Tooth #19
Diagnosis: Patient had pain when chewing . Pulp Necrosis with Symptomatic Apical PeriodontitisThis is a less common variety of molar, called Radix Entomolaris -> The distal has a second independent root in the lingual aspect.
The flexibility of ExactTaper H DC is valuable when treating these teeth, as the radix root is often severely dilacerated in a L-B dimension.
 |
 |
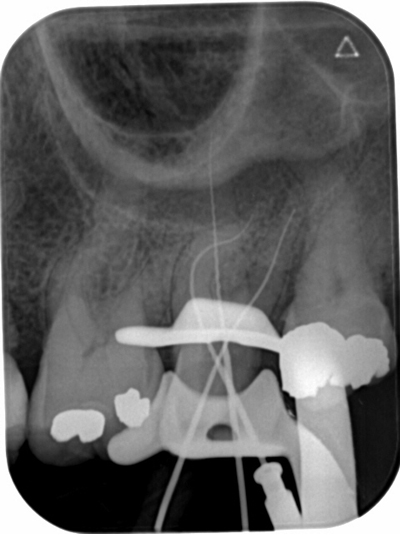
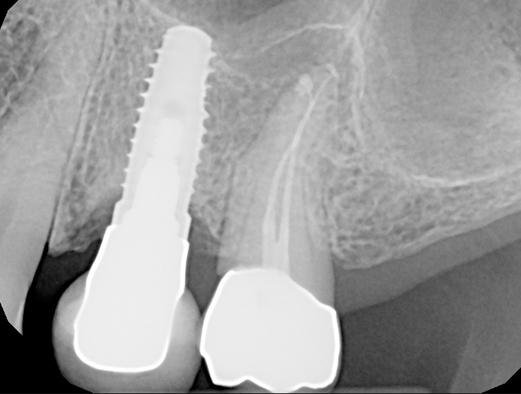
Case#3:
Tooth #13
Diagnosis: Patient presented with swelling in the B vestibule with intense pain. Pulp Necrosis with Acute Apical AbscessThe concern here is the lack of posterior support for this patient. The presence of an implant anterior to this terminal tooth highlights the additional risk factors this patient has for a successful outcome in the long-term. We must be cognizant of these not-so-obvious factors and tailor a treatment design around the concept of maximum longevity. The ExacttaperhDC file system with its preservation of PCD provides an ideal way to maintain structural integrity.
 |
 |
 |
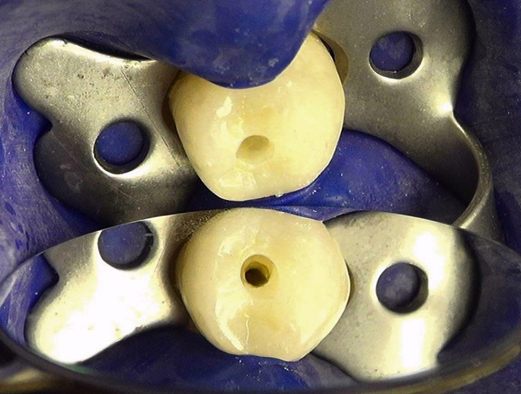
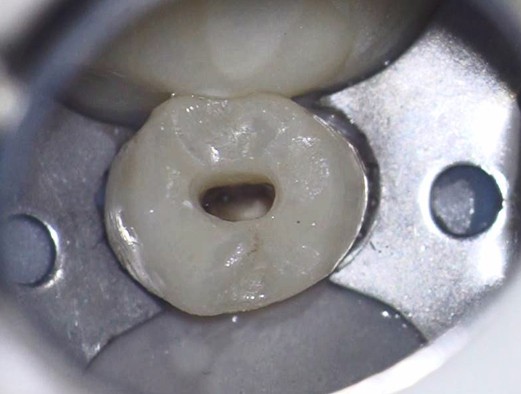
Case#4:
Tooth #29
Diagnosis: Patient had very little discomfort. Patient was placed in temporary crown after all caries excavated. Asymptomatic Irreversible Pulpitis secondary to decay with Normal peri-apex. This is a classic and easy example of a orifice directed access design. Basically, the shortest viable path to the canal orifice will determine the access design for this tooth.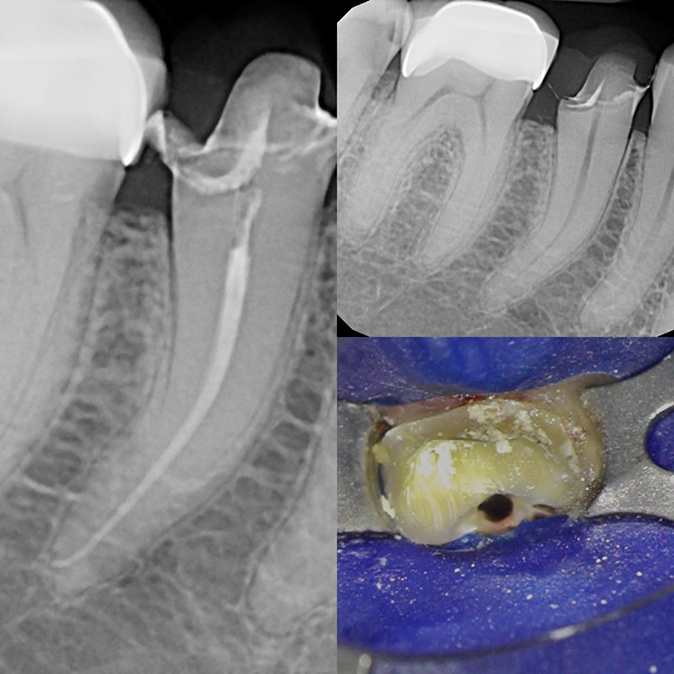 |
 |
Dr. Bobby Nadeau
Dr. Bobby Nadeau graduated with a DDS degree from Dalhousie University and earned a Master of Science in Endodontics from the University of Toronto. He has developed particular interests in Dynamic Navigation for Endodontics, Ergonomics in Microscope Dentistry, Restoratively Driven Endodontics, Clinical Decision Making and Dentin Conservation. Dr. Nadeau is in full time private practice in Kingston, Ontario, Canada. |
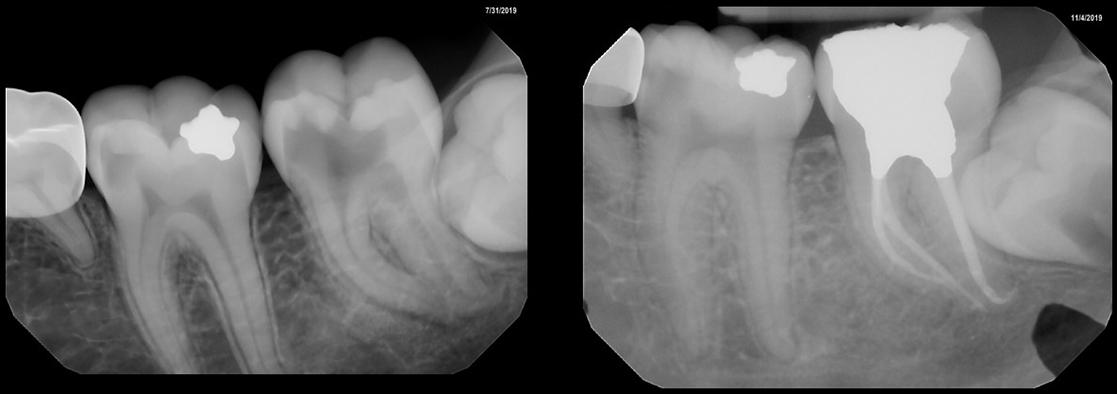
Case#1:
Tooth #14
Diagnosis: Pulp Necrosis with Symptomatic Apical Periodontitis. Treatment was completed in 3 visits with inter-appointment calcium hydroxide medicament.Glide path and working lengths obtained with #10 K-file. Instrumentation sequence: DCTaper™ #14/.03 @ 100 RPM, DCTaper™ #17/.04 @ 150 RPM and DCTaper™ #20/.06 @ 150 RPM.
At the 2nd visit, the patient still had some percussion sensitivity. A decision was made to instrument to DCTaper™ #25.06 in all canals.
Patient was completely asymptomatic at the 3rd visit. Obturation was completed with warm vertical compaction of gutta percha and AH+ Sealer. Permanent composite resin was immediately placed. Post-operative radiograph shows maintenance of the peri-cervical dentin and maintenance of original canal curvatures.
The tooth was referred back to the referring dentist for cuspal coverage.
 |
 |
Case#2:
Tooth #3
Diagnosis: Symptomatic Irreversible Pulpitis with Symptomatic Apical Periodontitis Treatment was completed in 2 visits with inter-appointment calcium hydroxide medicament. Glide path and working lengths obtained with #10 K-file. Instrumentation sequence: DCTaper™ #14/.03 @ 100 RPM, DCTaper™ #17/.04 @ 150 RPM and DCTaper™ #20/.06 @ 150 RPM.Patient was completely asymptomatic at the 2nd visit. Obturation was completed with warm vertical compaction of gutta percha and AH+ Sealer. Permanent composite resin was immediately placed. Post-operative radiograph shows maintenance of the peri-cervical dentin and maintenance of original canal curvatures. The tooth was referred back to the referring dentist for cuspal coverage.
 |
 |
 |
Dr. Yehuda Isseroff
Yehuda Isseroff is a graduate of Columbia University College of Dental Medicine, for both his DDS and post-graduate endodontic degrees. He resides in Bergenfield, NJ with his wife and three children, and is the owner of Bergen Endodontic Care in New Milford, NJ. When he's not with patients, Yehuda can usually be found on the tennis court or enjoying the great outdoors. |
Case#1:
17 y/o Female
presented initially as an emergency with #18 symptomatic irreversible pulpitis, symptomatic apical periodontitis due to deep decay. At the emergency visit, a pulpectomy was completed but no patency was achieved in any canal due to the extreme curvatures and time constraints. At the second visit, the tooth was more comfortable but still symptomatic to percussion. Patency was achieved in the mesial canals, but the apex of the distal canal still could not be reached, and calcium hydroxide was placed once again as deep as possible in an effort to help dissolve the tissue and open a glide path. At the third visit, the tooth was asymptomatic, and patency was finally achieved in the distal canal with a #10-C file and #15K file, and canals were cleaned/shaped to #25/v.06 DC Taper file.The canals were obturated with gutta percha and AH plus, and the core restored with amalgam. The post-operative radiograph illustrates the ability of the DC Taper file to manage even the sharpest and deepest of curves.
 |
Case#2:
66 y/o
presented with #31 which had a previous crown but had been lost for three months. The tooth was vital and asymptomatic, but required pre-prosthetic root canal therapy due to inadequate retention of the core. At the first visit, the distal was cleaned to DC Taper #30/v.06 and the mesials to a #25/v.06, and the tooth temporized. A small soffit of dentin was left over the mesial orifices to aid in retention of the future core. At the second visit, the tooth was asymptomatic, and the canals were obturated with GP and AH plus, and the post and core was completed with two Markley wires and Build-It. The patient soon returned to his general dentist for new crowns on #30 and #31. This case shows the ability of the DC Taper files to be precurved prior to entering the orifices, and still maintain the original canal curvatures throughout cleaning and shaping.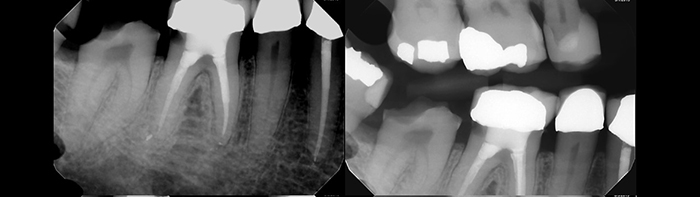 |
 |
Case#3:
57 y/o Male
presented with an asymptomatic but broken down #3. The tooth required pre-prosthetic RCT due to inadequate retention. At the first visit, an MB2 was located close to the palatal orifice, indicating a fully independent canal. At the second visit the case was completed with DC Taper files, #30/v.06 P, #25/v.06 MB/DB, and #20/v.06 MB2, the canals were filled with GP and AH plus, and the post/core with Markely wire and Build-It. The post-operative radiograph shows the flexibility and conservative ability of the #20 DC Taper file to shape MB2 canals with surprising locations!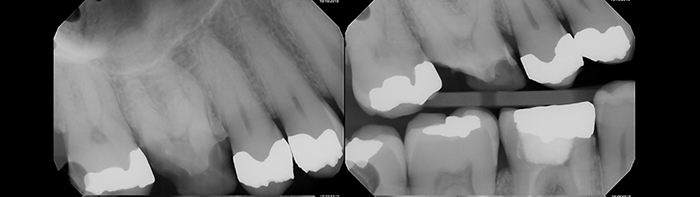 |
 |
Case#4:
34 y/o Female
with #11 symptomatic irreversible pulpitis due to a deep composite restoration. The case was completed in one visit with DC Taper #30/v.06 and composite resin to seal the access. This case illustrates how even in a long root, the DC Taper conserves the coronal dentin and maintains its original shape and curvature.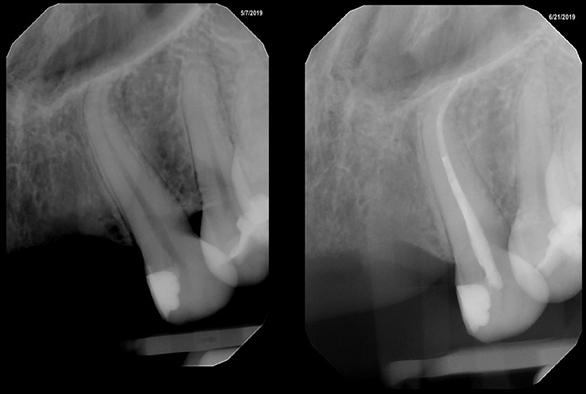 |
